Over the years, I have volunteered my expertise to help raise money for AIDS research and awareness. I have been involved with many programs for more than a decade, including California AIDS Ride, AIDS LifeCycle and Shifting Gears. I have treated thousands of cyclists ranging from elite-level racers to those who have never previously been on a bike.
The AIDS LifeCycle usually takes place during the first week of June and begins in San Francisco and ends in Los Angeles. The medical teams truly are integrated and working together in this moving city of cyclists, staff and volunteers. This ride inspires camaraderie and friends for life. It's an example of the way the world should be.
Along with these cyclists come injuries, most of which can be prevented. In this article, I will discuss the progression of knee injuries seen over seven consecutive days. One of the common, early signs of overuse is knee pain just below the patella (kneecap). By days three and four, this pain progresses to the lateral side of the knee and the low back - iliotibial band syndrome. Of course, muscle compensation plays a role by days four, five and six, and the medial side of the knee, the vastus medialis oblique (VMO), begins to hurt.
The training demands of these cyclists range from none to training one year out. But the common thread among many of these riders, regardless of their cycling level, is that they will develop knee pain. More of the elite-level riders usually do not start to get symptoms until days four, five and six. Less-conditioned riders tend to start getting symptoms of knee pain by day two, if not already from previous training.
These injuries are considered an overuse neuromuscular response, arising from either excessive use of an unconditioned, agonistic muscle in a very short period of time or repetitive agonistic use of a muscle over a long period of time. For these riders, integrated modalities were used at various stages of injuries. I followed 79 riders who were treated on a daily basis over the seven days. Treatments included combinations of ultrasound, taping, tuina, Chinese liniments, acupressure, auricular therapy and Chinese herbal medicine. Of these riders, 77 finished the ride with minimal soreness and two were unable to finish the ride.
Anterior knee pain is one of the most common conditions treated in this particular setting. The two most common are patellofemoral pain and patellar tendonitis. Both of these conditions are the result of agonistic neuromuscular overuse, with signs/symptoms surrounding the patella. (In this article, I am only focusing on progressive neuromuscular compensations from overuse.) In these 79 subjects, overuse injuries were the predominant factor of all these preventable target areas of pain, soreness and/or injury.
Biomechanical Mechanisms
When cycling, the hip, knee and ankle joints are synergistically working together. These joints will respond to neuromuscular compensations associated with the neuromuscular tightness (agonistic movements). Of course, all are dependent upon how one is sitting on the seat and the position of the foot while cycling. Over time, improper positioning can lead to neuromuscular imbalances that cause a variety of muscular compensation patterns. The key is to identify and anticipate where these compensation patterns are and treat them accordingly - before pain or other symptoms occur.
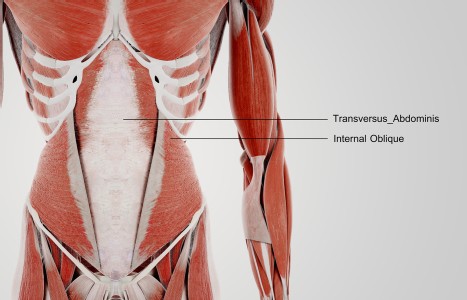
This neuromuscular tightness (excessive shortening) creates muscle imbalances and puts stress upon structures surrounding the patella, which causes pain. These neuromuscular imbalances create weaknesses in the VMO, vastus lateralis (VL), IT band (gluteus maximus and TFL) and the patellar tendon. The causative factors were: increased daily mileage (between 50 and 102 miles), hill work, biomechanical positioning of toe clips, seat adjustments and ride-duration fatigue.
Within sports medicine, the mechanism of injury involves physiological responses of the neuromuscular tissue to excessive agonistic movements of flexion/extension of the hip and knee joints, with slight internal or external rotation of the knee. This is dependent upon each cyclist's toe-clip position and neuromuscular compensation. Essentially, the neuromuscular response of agonistic contractions stemmed from overuse of the quads, gluteals, and/or hamstrings producing stress upon the structure surrounding the patella (iliotibial band, vastus lateralis, biceps femoris and vastus medialis). These muscles can pull the patella laterally, and due to the neuromuscular imbalance of the surrounding structures of the patella, pain may be felt medially and/or laterally, depending upon the individual and their natural biomechanical gait, stress, compensation and fatigue factors.
Kinesiology
The agonistic hip flexors include the iliopsoas, rectus femoris tensor fascia latae, pectineous and sartorius. The gluteus maximus, bicep femoris, semimembranosus, semi-tendinosus, and external rotators are responsible for hip extensors. In many cases, novice riders experience lateral knee pain at the attachment of the iliotibial band and/or knee pain just below the patella. Later, as the cyclist increases mileage and/or hill climbing, this pain will become more predominant, as neuro-muscular compensation responds to agonistic contractions and fatigue compensation patterns.
The agonistic knee flexors include the bicep femoris, semi-membranosus, semitendinosus, sartorius, gracilis, popliteus and gastrocnemius. The neuromuscular compensation is the result of the excessive agonistic movements, which create neuromuscular compensation patterns with the glutes and iliotibial band. The knee extensors (rectus femoris, vastus lateralis, vastus medialis and vastus intermedialis) tend to trigger agonistic contractions at the patellar tendon so pain is present just below the patella. This is known as patellar tendonitis.
Agonistic ankle-joint movers while the rider pedals involve plantar flexion and dorsi flexion. The associated muscles contractors include the gastrocnemius, flexor digitorium longus, flexor hallicus longus, peroneus longus, peroneus brevis, plantaris, soleus and tibialis posterior. Especially with novice cyclists, the neuromuscular agonistic component primarily involves ankle plantar flexion in the downstroke on the pedal. With more experienced and/or elite cyclists, the pedaling emphasis also is placed on the upstroke, involving dorsi flexors as tibialis anterior, peroneus tertius, extensor digitorium longus, and extensor hallicus longus.
Environmental Conditions
Athletes were exposed to the elements around the clock, from freezing temperatures in the early hours of the morning to 90 degrees by 2 p.m. Some of these cyclists were HIV-positive or had AIDS. Although these individuals have seemingly good constitutions, it was assumed they were susceptible due to decreased immune system response. There were shower facilities, but athletes slept in tents overnight and had to get on the road by 6:30 a.m. In Chinese medicine, this plays a role in part of the diagnostic method of six external pathogens associated with bi syndromes, wei qi deficiency due to pre-existing LG qi, Sp qi deficiency, damp accumulation, and Liv qi stagnation.
Chinese Medicine
According to the Oriental philosophy, the primary pathological mechanisms are blood and qi stagnation, due to overexertion, with further susceptibility to the invasion of wind, cold, and damp affecting the channels externally and organs internally. This results in decreased nourishment to the sinews and bones. Of course, the manifestation of pathogenic factors varied individually. These particular cyclists initially developed stagnation of qi/blood and, subsequently, liver qi stagnation. As the ride progressed, excessive physical exertion created deficiency patterns, if not already present due to previous preparation training, resulting in system depletion or further deficiency of kidney qi/yin deficiency and spleen qi deficiency.
However, another aspect that needs to be considered is that excessive physical overexertion consumes the zheng qi, which can result in a lowered resistance. With excessive physical exertion over the first three days, internal deficiency conditions started to become more apparent involving the following patterns: wei qi deficiency, Sp qi deficiency, Liv/K qi deficiency, K yin and yang deficiency. Channel and organs became susceptible to invasion of wind, cold and damp due to the environmental conditions these riders endured on a daily basis. Deficiency of qi and blood was predicable for lowered resistance, allowing the invasion of the six exogenous pathogenic factors.
Some examples of treatments implemented included moxa over channels/meridians/vessels, along with tuina and PNF. Herbal formulas and magnets were given to those athletes for deficiency conditions to improve blood and qi deficiency (R12, St36, Sp6/ba zhen wan), to prevent further deficiency from the overexertion of riding seven consecutive days. Those who were susceptible to wind, cold and damp bi syndrome were given herbs in the morning and late afternoon (du huo ji sheng wan/chai ge jie ji wan). Those with autoimmune conditions were counterbalanced with herbal formulas and magnets to address the pre-existing Sp qi deficiency (St36, Sp6, R6, R12/bu zhong yi qi wan) sheng ma wan, wu jia shen pian, LG qi deficiency (LG7, K6), K qi (UB23, K3 and K6, Liv8), yin/yang deficiency (Yin Def K3/liu wei di huang wan/jing qi wan; Yang Def K3, D4, UB23 w/moxa/you gui yin/jia jian jin gui shen qi wan), among other conditions during their training prior to the ride. All treatments took less than 15 minutes to implement and were highly effective.
If they could not take herbs, then magnets were used after implementing EAS/PENS using microcurrent, with point combination from above. This was done before bedtime. Constant counterbalancing of muscular biomechanical compensations was addressed individually, as well as TCM diagnostic strategy in anticipation of potential injuries from pattern and channel/vessel/meridian differentiations, along with orthopedic and muscular compensation assessments. Others were simply pulled from the ride due to the severity of physiological manifestations presenting at the time.
In the sports medicine arena, most practitioners do their work after the injury already has occurred. This makes it difficult to practice prevention, even if patients are given "home exercises," because if pain is present, depending upon severity, we can only prevent the injury from getting worse. This scenario also is the typical mindset within Olympic and professional sports.
The key is to identify and anticipate where these compensation patterns are and treat them accordingly before pain or the symptom occurs. This is difficult because there are a variety of ways to prevent these compensation patterns. One of the easiest is stretching, but getting the riders to stretch is rather difficult if pain is not present. This is a double-edged sword in education and application. The other dilemma is using Oriental medicine as prevention rather than after the injury has occurred. This is particularly due to lack of understanding of what Oriental medicine has to offer athletes/patients in general. However, compliance with treatment (when signs/symptoms are not present) really is no different than stretching before the race.
Oriental medicine's approach is considered "external injuries," which mainly stem from martial arts injuries. Here in the U.S., this approach, unfortunately, still is considered "unconventional," although this mindset is changing.
To be successful in this type of environment, it is imperative that the acupuncturist has an extensive knowledge of sports medicine and Chinese medicine before implementing integrated treatment principles. For optimal results with Eastern and Western treatment philosophies, it is critical that there is a mutual understanding when working with a medical team. Due to the large volume of cyclists treated, traditional acupuncture treatments were not implemented for these cases. One year, I was able to implement acupuncture treatments for an outbreak of diarrhea using UB25, St25, St36, Sp6, Sp9, St44, and LI4. This protocol was very effective, to the amazement of the medical doctors observing.
The time constraints in treating these cyclists are unusual, along with the treatment areas being outside, in tents. When assessing cyclists with these different types of knee conditions, one must be able to make expedient treatment decisions. By integrating these medical philosophies and treatments, we prevented patellar tendonitis, VMO and patellofemoral pain with excessive neuromuscular agonistic movements for 77 cyclists. I encourage more research to be conducted. As part of the sports medicine team, our goals should always be injury prevention strategies and ultimately, enhanced athletic performance. The biggest dilemma with this mindset is how to develop evidence-based quantification when the injury has yet to occur.
Editor's note: I would like to thank all of the CAR & ALC riders, volunteers and staff for their efforts over the years.
Resources
- Zachazewski J, Magee D, Quillen W. Athletic Injuries and Rehabilitation. Philadelphia: W.B. Sanders, 1996; pp. 703-4.
- Yan Cui-lan, Zhu Yun-long. The Treatment of External Diseases with Acupuncture & Moxibustion. Boulder, CO: Blue Poppy Press, 1997.
- Cheng Dan-An, Wu Ming. Acupuncture and Moxibustion Formulas & Treatments. Boulder, CO: Blue Poppy Press, 1996; pp. 165-7.
- Vangermeersch L, Sun Pei-Lin. Rheumatic Disorders Treated by Traditional Chinese Medicine. Brussels: SATAS, 1994; pp. 19-23.
- American Academy of Orthopedic Surgeons: Athletic Training and Sports Medicine. Park Ridge, IL: 1991; pp. 322-40.
- Qing-Fu Hu: "The Practice of Acupuncture and Herbal Therapies (I)," Oriental Healing Arts Institute, April 18, 1999, Irvine, CA.
- Ross J. Acupuncture Point Combinations: The Key to Clinical Success. New York: Churchill Livingstone, 1995, pp. 170-266.